TL;DR:
- A USMLE percentile rank indicates your relative standing among first-time examinees from accredited U.S. and Canadian medical schools. It influences residency program screening more than most students realize, with higher percentiles improving match prospects.
A USMLE percentile rank is defined as your relative standing among first-time test-takers from LCME-accredited U.S. and Canadian medical schools during a fixed reference period. Understanding what does USMLE percentile mean is not just an academic exercise. Your percentile directly determines whether a residency program's screening algorithm advances your application or stops it cold. The official USMLE Score Interpretation Guidelines publish norm tables for Steps 2 CK and 3, and every medical student should read them before interpreting any score report.
What does USMLE percentile mean and how is it calculated?
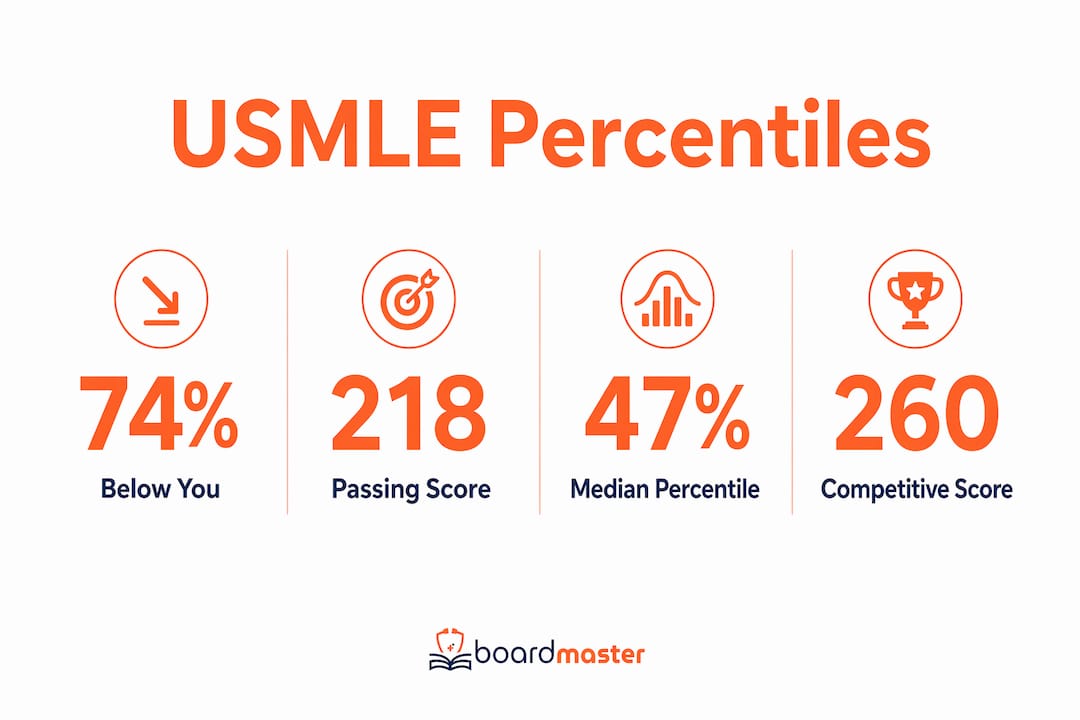
A USMLE percentile tells you what percentage of the reference cohort scored below you. If you land at the 74th percentile, 74% of first-time U.S. and Canadian test-takers scored lower than you did. That single number carries more weight in residency screening than most students realize.
The calculation starts with your three-digit scaled score. USMLE uses a statistical process called equating to adjust for difficulty differences across exam forms. Equating means a student who took a harder version of the exam is not penalized compared to someone who took an easier version. Your scaled score is then compared against the reference cohort to produce a percentile rank.
A few critical facts about the norm group:
- The reference cohort is limited to first-time test-takers from LCME-accredited U.S. and Canadian schools only.
- The cohort is measured over a defined multi-year period, not a single calendar year.
- The mean score for the 2023–2024 cohort was approximately 249–250, placing it at the 50th percentile.
- Step 1 is now pass/fail. No percentile is reported for Step 1.
- Official norm tables exist for Steps 2 CK and 3 only.
Pro Tip: Your percent correct on a question bank does not translate directly to your official scaled score or percentile. Question bank percentages and official USMLE scores use entirely different equating methods. Never use your question bank percentage to predict your percentile.
The types of USMLE performance metrics that appear on your score report are more nuanced than a single number suggests. Reading the official guidelines is the only reliable way to interpret them correctly.
What do USMLE percentiles mean for your exam performance?
Percentile brackets tell you where you stand competitively, not how much medicine you know. A student at the 24th percentile may understand pharmacology deeply but struggled with test-taking strategy on exam day. The percentile reflects performance relative to a cohort, not absolute clinical competence.
The score-to-percentile relationship for Step 2 CK is not linear. Small score differences in the middle of the distribution can produce large percentile jumps. The table below shows key benchmarks:
| Step 2 CK Scaled Score | Approximate Percentile | Competitive Signal |
|---|---|---|
| 218 (minimum passing) | ~2nd percentile | Passed; very limited specialty options |
| 240 | ~24th percentile | Below average; competitive for fewer programs |
| 250 | ~47th–50th percentile | Average; broadly competitive |
| 260 | ~74th percentile | Above average; competitive for most specialties |
| 265+ | ~85th+ percentile | Highly competitive; opens selective programs |
These benchmarks come from official score interpretation data. The minimum passing score of 218 corresponds to roughly the 2nd percentile, meaning nearly every test-taker in the reference cohort scored higher. Passing is not the same as competitive.
The jump from 240 to 250 moves you from the 24th to the 47th percentile. That is a 23-percentile-point gain from just 10 scaled score points. This compression effect means that targeted preparation in the middle of the score range produces outsized percentile gains.
Pro Tip: Focus your preparation on your weakest high-yield content areas rather than reviewing topics you already know well. Moving from 240 to 250 is far more achievable than moving from 260 to 270, and it produces a much larger percentile gain relative to the effort invested.
Understanding your three-digit USMLE score in relation to your percentile gives you a clearer picture of where you actually stand in the applicant pool.
How do USMLE percentiles affect residency applications?
Step 2 CK percentiles now carry the most weight in residency screening. Since Step 1 became pass/fail, 83% of residency program directors rely on Step 2 CK scores to evaluate applicants, and 30% use explicit score thresholds to filter interview invitations. That means your percentile rank is often the first thing a program sees before reading a single word of your personal statement.
The practical impact varies by specialty:
- Highly competitive specialties (dermatology, orthopedic surgery, plastic surgery) typically expect scores in the 260+ range, placing applicants above the 74th percentile.
- Moderately competitive specialties (internal medicine, pediatrics, family medicine) are more flexible, but scores below the 24th percentile still raise flags.
- Less competitive specialties may accept scores closer to the mean, but a below-average percentile still limits program choice.
- International medical graduates face stricter thresholds at most programs, making a high Step 2 CK percentile even more critical for clearing initial filters.
A high Step 2 CK percentile clears the screening filter, but it does not guarantee an interview or a match. Program directors conduct holistic reviews that weigh clinical evaluations, letters of recommendation, research experience, and personal statements alongside the score. A student at the 85th percentile with weak clinical grades faces real competition from a student at the 65th percentile with exceptional evaluations.
The takeaway is direct: your percentile gets your application read. Everything else determines whether you match.
What are common misconceptions about USMLE scoring and percentiles?
Several widespread misunderstandings cause students to misread their scores and make poor preparation decisions. Knowing these pitfalls protects you from chasing the wrong targets.
Percentiles are not fixed. The cohort changes with each reporting period. A score of 250 may correspond to the 47th percentile today and a slightly different percentile in a future cycle. Percentiles change dynamically as cohort performance shifts, so always consult the current official guidelines rather than tables posted on forums or outdated websites.
You cannot compare percentiles across Steps. Step 2 CK and Step 3 scores are scaled differently. A score of 250 on Step 2 CK does not correspond to the same percentile as 250 on Step 3. Each exam has its own norm table, and cross-Step comparisons are meaningless.
Small score changes rarely move the needle. A 2–4 point score increase typically produces a negligible percentile shift. Jumps of 6+ points are generally needed to reflect a meaningful competitive improvement. Students who obsess over minor score fluctuations between practice tests are tracking noise, not signal.
Question bank percentages are not percentiles. Getting 70% correct on a question bank does not mean you are at the 70th percentile. Percent correct on question banks does not correlate directly to official scaled scores because the equating process is complex and exam-specific.
Percentiles measure relative performance, not competence. A percentile tells you where you rank in a cohort. It does not measure how good a physician you will be. Percentiles reflect relative exam performance and should never be treated as an absolute measure of medical knowledge.
Key Takeaways
Your USMLE percentile rank is a relative measure that compares your scaled score to first-time LCME-accredited test-takers, and Step 2 CK percentiles now serve as the primary numeric filter in residency screening.
| Point | Details |
|---|---|
| Percentile definition | Your rank shows what percentage of the reference cohort scored below you. |
| Step 1 has no percentile | Step 1 is pass/fail only; percentile tables apply to Steps 2 CK and 3. |
| Score-to-percentile benchmarks | A score of 240 is ~24th percentile; 250 is ~47th; 260 is ~74th percentile. |
| Residency screening impact | 83% of program directors use Step 2 CK scores, with 30% applying score cutoffs. |
| Percentiles are dynamic | Always consult current official USMLE guidelines, not outdated forum tables. |
Why I think students misuse percentile data more than any other metric
Students treat their USMLE percentile like a final verdict. I have watched students with a 260 spiral into anxiety over a 2-point drop on a practice test, and students with a 245 give up on competitive specialties before the application cycle even opens. Both reactions are driven by misreading what a percentile actually tells you.
A percentile is a snapshot of relative performance at one point in time, against one specific cohort. It does not predict your ceiling. The students I have seen make the biggest gains are the ones who stop comparing themselves to a norm group and start asking a more useful question: which specific content areas are costing me points?
The psychological trap is real. When you see a percentile number, your brain treats it as a permanent label. It is not. Cohorts shift, preparation strategies improve, and a focused 6-week study block targeting your weakest systems can move you 10+ scaled score points, which at the midrange of the distribution translates to a dramatic percentile jump.
My honest advice: check your percentile once when you receive your score report, use it to calibrate your specialty list, and then stop looking at it. Put your energy into the factors you can still control: clinical evaluations, research, and targeted preparation for any remaining Steps.
— Dr. Ahmed Abuzoor
How BoardMaster helps you target the percentile gains that matter
Knowing your percentile is one thing. Knowing exactly which content gaps are holding your score down is another.
BoardMaster generates USMLE-style practice questions directly from your lecture notes, so your study time targets the concepts your professors emphasize rather than generic content that may never appear on your exam. One student, Sarah, moved from the 73rd to the 92nd percentile while cutting her study hours in half by focusing exclusively on high-yield material identified through BoardMaster's question generation. Watch the AI question generator in action to see how targeted preparation translates into real percentile movement. Medical schools looking to support their students at scale can also explore BoardMaster's partnership program for institution-wide access.
FAQ
What does a USMLE percentile rank actually mean?
A USMLE percentile rank shows what percentage of first-time test-takers from LCME-accredited U.S. and Canadian schools scored below you during a defined reference period. A 74th percentile means 74% of that cohort scored lower than you.
Does Step 1 have a percentile?
No. Step 1 became pass/fail, so no percentile rank is reported for it. Percentile tables apply only to Steps 2 CK and 3.
What Step 2 CK score is considered competitive for residency?
A score of 250 places you near the 47th–50th percentile, which is broadly competitive. Scores of 260 and above, corresponding to roughly the 74th percentile, are considered strong for most specialties.
Can I compare my Step 2 CK percentile to my Step 3 percentile?
No. Step 2 CK and Step 3 use different scaling methods, so the same scaled score produces different percentiles on each exam. Always use the exam-specific norm table from the official USMLE Score Interpretation Guidelines.
How much does my score need to change to improve my percentile meaningfully?
A change of 2–4 scaled score points typically produces a negligible percentile shift. A jump of 6 or more points generally reflects a meaningful competitive improvement worth noting in your application strategy.